fPAES
Diagnostics for fPAES
CECS
Diagnostics for CECS
Treatment
What is Functional Popliteal Artery Entrapmant?
If you've come to this blog to learn more about Functional Popliteal Artery Entrapment Syndrome (fPAES), at this point in your google searches, you probably know the basics about PAES. Popliteal Artery Entrapment Syndrome is exactly what it sounds like: Entrapment of the Popliteal Artery. The popliteal artery is the artery that runs directly behind the knee and supplies your lower legs with blood. Remember your high school anatomy; Arteries carry the blood that flows from the heart and that supplies all the necessary nutrients to the muscles and tissue of the body.
In my experience, most practitioners you will see to potentially receive this diagnosis only know the general umbrella of PAES, but there are actually 6 types! Understanding the difference between the functional type and all the others is key to knowing how to advocate for yourself and to make sure you get the testing you deserve! Five of the 6 types of Popliteal Artery Entrapment are what are referred to by those that know the difference as "anatomical popliteal artery entrapment" meaning that there is a clear anatomical abnormality that can be detected in a CT or MRI relatively quickly (so I hear, but no doubt it's still a vastly unrecognized condition and even getting to appropriate scanning can be difficult)
In my experience, most practitioners you will see to potentially receive this diagnosis only know the general umbrella of PAES, but there are actually 6 types! Understanding the difference between the functional type and all the others is key to knowing how to advocate for yourself and to make sure you get the testing you deserve! Five of the 6 types of Popliteal Artery Entrapment are what are referred to by those that know the difference as "anatomical popliteal artery entrapment" meaning that there is a clear anatomical abnormality that can be detected in a CT or MRI relatively quickly (so I hear, but no doubt it's still a vastly unrecognized condition and even getting to appropriate scanning can be difficult)
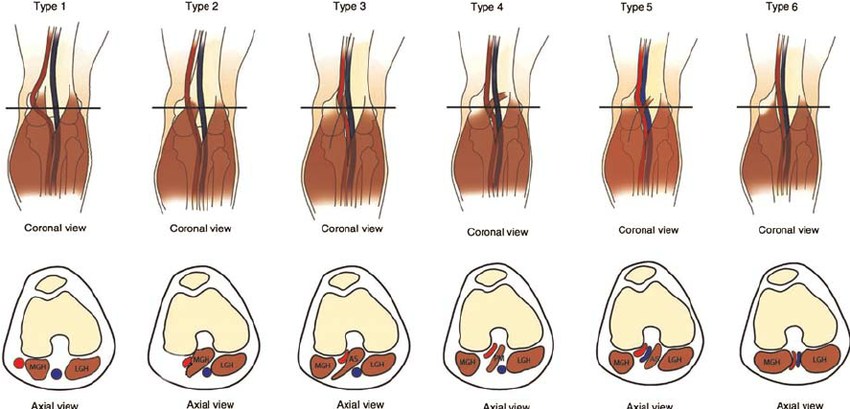
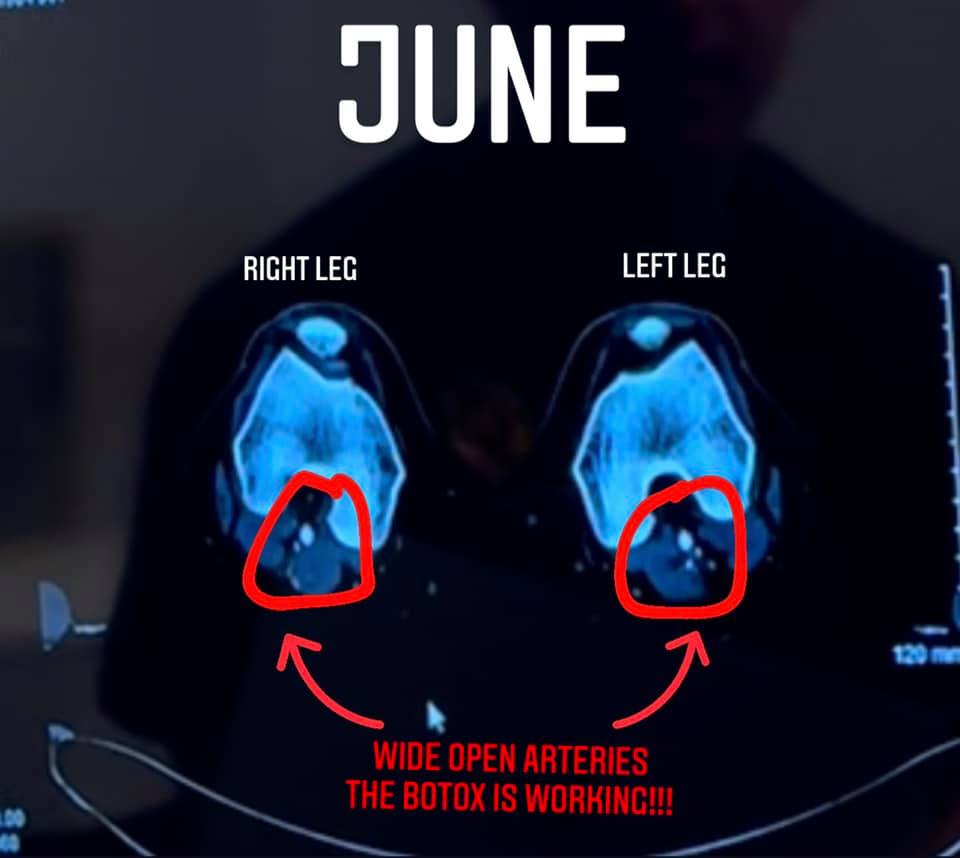
The first 5 types you can clearly see that there is a band of muscle in the way or that the artery is just not in the right spot. In type 6 everything is in the normal spot, however with the flexed muscles you get compression. It's easiest to view that compression with the Axial view. For anyone that doesn't know how to view that, this is pretty important for when I show my own images later. You are basically looking at a slice of the leg as if you are looking up through the feet. The off-white oval at the top is the patella, and then you can see the bone in that horseshoe shape. Below that you see the small blue and red circles (or in type 6 the flattened little oval shapes) of arteries and veins and then you see the muscles. I don't actually know how to read scans, but have learned a little over time to help me understand my own struggles.
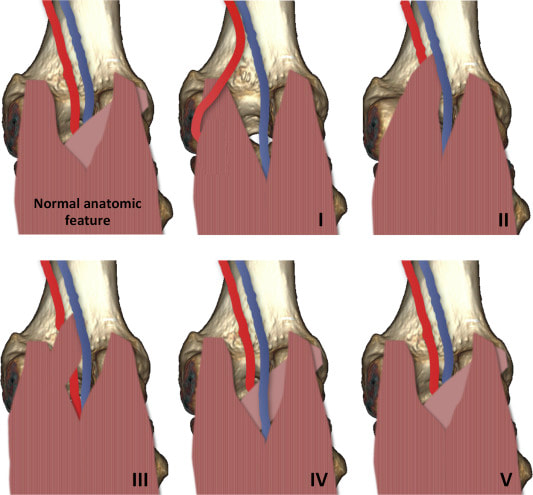
What makes the type 6 so hard to diagnose is that some people don't even know about it! Here's another picture of different types of PAES. I took this image from another journal published in 2016 (click picture for link) and functional wasn't even included! If you're wondering what functional looks like at rest, Check out the image labeled "normal".... and therein lies the difficulty getting diagnosed with fPAES. Most of the time we are getting our imaging done at rest! Lets go over some of the imaging you might receive in the hunt for this diagnosis.
Diagnostics for Functional Popliteal Artery Entrapment
X-Rays
I have never been diagnosed with anything using an x-ray.... except maybe something related to my wisdom teeth. Even stress fractures aren't always detected on an x-ray but it's quick, results are immediately available, and it's billable to insurance. It seems like a necessary step to getting the next level of testing: an MRI.
MRI
I've had so many MRI's across my running career. They are painless and only mildly annoying (unless you're getting a brain MRI, 10/10 don't recommend). MRI's can even detect previous injuries that have healed. Remember, though, that at rest functional popliteal artery entrapment is "normal" so if you're doing a "normal" MRI, they wont find anything. Another difficulty with the MRI for this particular issue, (for me anyway), is the lack of blood flow to my calves caused me to actually tear my calf. My muscles were starved of oxygen and nutrients so they were 1. not healing very well between "episodes" 2. extremely fragile. So my MRI showed "torn gastroc and soleus" which to a doctor, that might seem like an answer to your problem "your calf is torn, you need rest and rehabilitation" it can prolong further testing, and actually make your condition worse! Do you want to know what your rehab is for a torn calf? Calf Raises. Do you want to know what the worst thing you can do for fPAES is? ... Calf Raises. I knew that the calf being torn was a symptom not a cause, so I kept looking.
I have never been diagnosed with anything using an x-ray.... except maybe something related to my wisdom teeth. Even stress fractures aren't always detected on an x-ray but it's quick, results are immediately available, and it's billable to insurance. It seems like a necessary step to getting the next level of testing: an MRI.
MRI
I've had so many MRI's across my running career. They are painless and only mildly annoying (unless you're getting a brain MRI, 10/10 don't recommend). MRI's can even detect previous injuries that have healed. Remember, though, that at rest functional popliteal artery entrapment is "normal" so if you're doing a "normal" MRI, they wont find anything. Another difficulty with the MRI for this particular issue, (for me anyway), is the lack of blood flow to my calves caused me to actually tear my calf. My muscles were starved of oxygen and nutrients so they were 1. not healing very well between "episodes" 2. extremely fragile. So my MRI showed "torn gastroc and soleus" which to a doctor, that might seem like an answer to your problem "your calf is torn, you need rest and rehabilitation" it can prolong further testing, and actually make your condition worse! Do you want to know what your rehab is for a torn calf? Calf Raises. Do you want to know what the worst thing you can do for fPAES is? ... Calf Raises. I knew that the calf being torn was a symptom not a cause, so I kept looking.
Doppler Ultrasound ABI
Another relatively painless test. You can expect to have cuffs put on your ankles to check your blood pressure before and after exercise. They will also take an ultrasound to try to find where the blood flow is slowed down... they will say they "provoked" your symptoms by having you press your toes into someones leg or onto a board that a person is holding, and they will check dorsi flexion and plantar flexion.... but knowing what I know now, it's no wonder everything came back normal for me, and it seems like that is the case for many people that are more fit and can recover quickly. "Provoked" symptoms is a loose term. Certainly isn't enough pressure to produce symptoms in my case and it seems in many other cases as well. Truth be told, I don't have a great understanding of this testing procedure, but what I do know for sure is that many people get false negatives, so don't consider this test "ruling it out"
Another relatively painless test. You can expect to have cuffs put on your ankles to check your blood pressure before and after exercise. They will also take an ultrasound to try to find where the blood flow is slowed down... they will say they "provoked" your symptoms by having you press your toes into someones leg or onto a board that a person is holding, and they will check dorsi flexion and plantar flexion.... but knowing what I know now, it's no wonder everything came back normal for me, and it seems like that is the case for many people that are more fit and can recover quickly. "Provoked" symptoms is a loose term. Certainly isn't enough pressure to produce symptoms in my case and it seems in many other cases as well. Truth be told, I don't have a great understanding of this testing procedure, but what I do know for sure is that many people get false negatives, so don't consider this test "ruling it out"
CTA
The CTA with contrast is another test that you may receive. This test was no fun for me the first time. I had to do it from my chest down because I was sent on a wild goose hunt looking for another diagnosis that shows up on the intestines, and I had to hold my breath during the test. Since then I've had multiple CTA's and they've been a little less nauseating. They inject a warm dye into your bloodstream, so when you feel that, it's pretty intense. I didn't get the warnings of feeling like I will pee my pants and vertigo for the first test. So be prepared for that... Again, it comes back to the same problem: AT REST everything is normal, so how accurate do you think this is? If you have anatomical PAES, it will show up here for sure (and I think the MRI as well, but I don't actually know) and that's the problem... this will pretty much rule out 5/6 types. You will read things on your report that say "unremarkable" and "normal"... but that is at rest. If you think you have this condition you must get these tests provoked... and really provoked. Not pushing gently against someones leg, but pushing full force!
The CTA with contrast is another test that you may receive. This test was no fun for me the first time. I had to do it from my chest down because I was sent on a wild goose hunt looking for another diagnosis that shows up on the intestines, and I had to hold my breath during the test. Since then I've had multiple CTA's and they've been a little less nauseating. They inject a warm dye into your bloodstream, so when you feel that, it's pretty intense. I didn't get the warnings of feeling like I will pee my pants and vertigo for the first test. So be prepared for that... Again, it comes back to the same problem: AT REST everything is normal, so how accurate do you think this is? If you have anatomical PAES, it will show up here for sure (and I think the MRI as well, but I don't actually know) and that's the problem... this will pretty much rule out 5/6 types. You will read things on your report that say "unremarkable" and "normal"... but that is at rest. If you think you have this condition you must get these tests provoked... and really provoked. Not pushing gently against someones leg, but pushing full force!
Intravascular Ultrasound or Angiogram
Okay, I never had these done and don't know much about them other than the fact that they are done by a vascular surgeon and billed as a surgery. They insert a camera through your groin I believe and send that camera through your arteries and veins. I am not sure if they provoke symptoms during but you are awake for it so that you can move a bit and you should be able to see what they are looking at. My dad had this done (fairly certain this thing is genetic and he was diagnosed incorrectly and treated by putting in a stent). From my understanding, though, this can still show up negative for functional types.
Okay, I never had these done and don't know much about them other than the fact that they are done by a vascular surgeon and billed as a surgery. They insert a camera through your groin I believe and send that camera through your arteries and veins. I am not sure if they provoke symptoms during but you are awake for it so that you can move a bit and you should be able to see what they are looking at. My dad had this done (fairly certain this thing is genetic and he was diagnosed incorrectly and treated by putting in a stent). From my understanding, though, this can still show up negative for functional types.
The McGinley Method: MVP Flex
I'm a little bias, but this is the way to go! Dr. McGinley patented the MVP flex, which is basically a plate to push on during your CTA. You have handles that are sized specifically to you and it really helps you pull and push your hardest. What I really like about it is that you can actually measure your output during the scan. The plate is attached to a little computer that reads how many pounds of pressure and you are instructed to keep that number above 120. Let me tell you, it's no wonder there are so many false negatives with other "provoked" tests! It is a WORKOUT to keep that number at 120! It is nice to have that very concrete target so that there is less margin of error during the treatment phases as well.
I'm a little bias, but this is the way to go! Dr. McGinley patented the MVP flex, which is basically a plate to push on during your CTA. You have handles that are sized specifically to you and it really helps you pull and push your hardest. What I really like about it is that you can actually measure your output during the scan. The plate is attached to a little computer that reads how many pounds of pressure and you are instructed to keep that number above 120. Let me tell you, it's no wonder there are so many false negatives with other "provoked" tests! It is a WORKOUT to keep that number at 120! It is nice to have that very concrete target so that there is less margin of error during the treatment phases as well.

There are other doctors that use a cloth that you hold and press into and people have seen results that way. McGinley comes with a high price tag so if you want to be more sure about your diagnosis before you make that commitment, make sure you get a CTA with full force effort! You need to be pressing so hard that you are breaking of sweat! Now that we've talked about diagnostics, it seems like treatment would be next, but before I do that I'm going to talk about Chronic Exertional Compartment Syndrome as the diagnosis's are so closely related!
Chronic Exertional Compartment Syndrome
Compartment Syndrome has been on my radar as a potential diagnosis for years. It can be thrown around vaguely for anyone experiencing ongoing lower leg pain or swelling. The "gold standard" (I say that lightly) test for it is a stryker test where they measure the baseline pressure in your compartments and then have you run a specific time on the treadmill, and then measure the pressure again. If it rises to a certain level then it's "compartment syndrome". This test is relatively invasive and apparently the needles are expensive (and big), and it's actually quite hard to find people to properly perform the test so in my experience a PT or an athletic trainer might just slap a good ol' "compartment syndrome" diagnosis to explain your symptoms and encourage rest and modified training. There is a difference between compartment syndrome caused by an accident or a blunt force (acute compartment syndrome), and the type I'm talking about (chronic exertional compartment syndrome)... I don't know much about acute. In light of new information, I'm glad I managed my symptoms on my own as long as I did in order to avoid potentially unnecessary surgeries.
It's 2021 as I'm writing this, and most people that have been treated surgically for compartment syndrome would describe it as a condition where the fascia is too tight or the compartments are too small to accommodate swelling of the muscles. This can cause painful pressure! While there is seed of truth to that, new research conducted by Dr. McGinley is showing a more specific cause (and you guessed it, it's related to fPAES). As the story goes, one of the technicians took a scan of someones legs a bit higher than normal, and veinous compression was discovered. McGinley has since discovered a strong correlation between compartment syndrome and compressed veins.
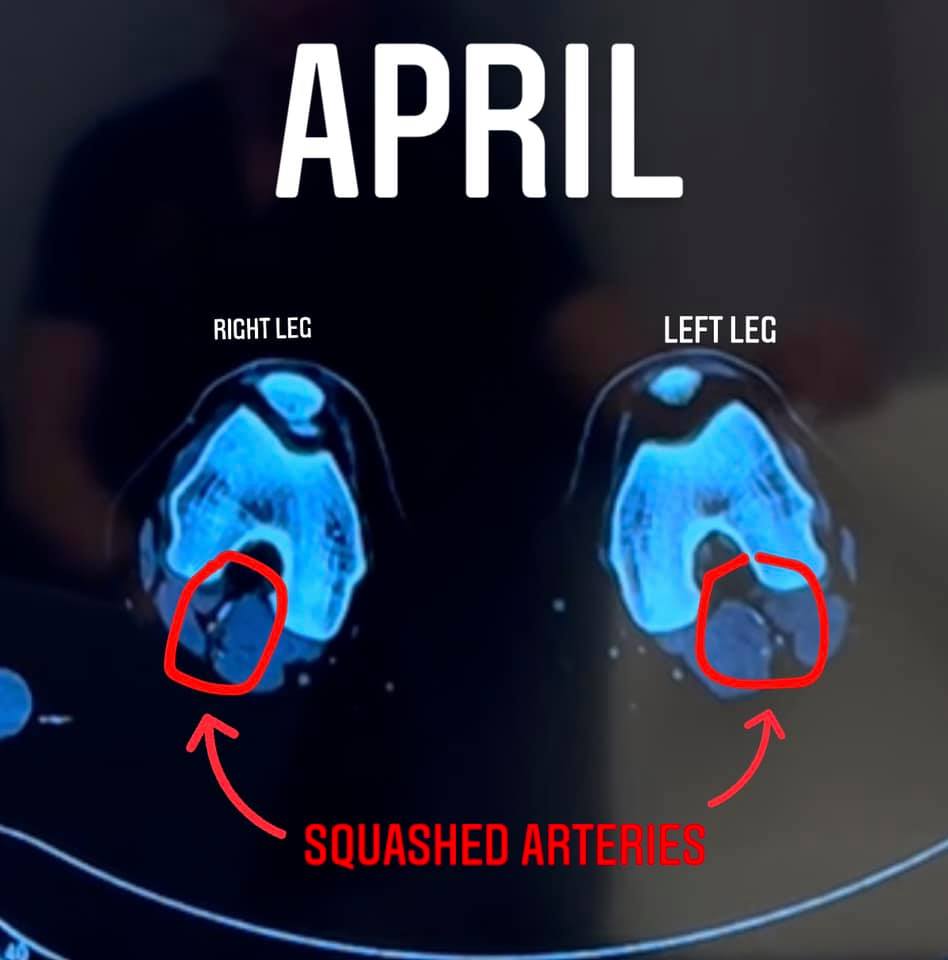
How I'm understanding it now is that remember: arteries carry the blood from the heart. So veins carry blood back to the heart. Remember that imaging of the flattened artery and vein in the back of the knee. If a flattened artery prevents blood from flowing down the leg, what happens when you flatten or compress a vein? Blood can't get back up. According to Dr. McGinley, arteries are much harder to compress than veins so there's a mismatch of blood flow and pressure and as a result extra fluid builds up in the lower legs and BOOM... Pain.
So it would seem the best way to get that pain to stop would be to stop the compression.
Diagnostics for CECS
Rule it all Out
The first thing typically done to diagnose compartment syndrome, is rule everything else out first. So you will get some of the same tests above: X-ray and MRI to make sure there's nothing more obvious going on. Maybe PT will be required, and even orthotics which I will discuss in treatment. Some doctors may even order blood tests to check and make sure all those numbers are in the normal range.
Stryker Test
It is not easy to get to the point where you actually have a doctor order the "Gold Standard" Stryker test. The Stryker test involves a hand held device that measures pressure in the 4 different compartments. Essentially you are going to have needles jabbed into your compartments before and after exercise as I mentioned above and then if your reading is above a certain number? Boom, you have compartment syndrome and they line you up for a pretty invasive surgery. It was incredibly difficult for me to get a Stryker test due to covid, but finally my best friend, who is an orthopedic surgeon, told me to drive 3 hours to her and that she would do the test. She doesn't perform them often and did everything right but noticed that the pressure reader was so sensitive. My pressure was already high enough for a CECS diagnosis before exercise and it barely elevated or changed after exercise so Chronic exertional Compartment Syndrome theoretically should get worse upon exertion and while my symptoms got worse, the pressure in my compartments didn’t rise. I’m not sure if this happens to all people with fPAES, but these results were strange. Since it was my best friend she didn’t want me to get surgery yet even though technically my numbers were high enough to indicate that was the next step, she did not like the results or the surgical outcomes for me and recommended I check with vascular before getting surgery since PAES was already on my radar. At the time all I wanted was a surgery, but she told me the outcomes of both surgeries weren’t good. I felt deflated because the only options on the table were either bad outcome surgeries or sedentary life. I was willing to take my chances with surgery because my symptoms were getting pretty severe that walking was pretty painful. I was having trouble getting anyone to see me due to COVID but eventually got in with vascular to see about PAES. I wont get into the craziness once I was on the vascular track as it's all in my blog, but all this to say, the Stryker test showed compartment syndrome, but my doctor felt that it wasn’t accurate or a reliable test due to pressure staying the same after exertion.
The first thing typically done to diagnose compartment syndrome, is rule everything else out first. So you will get some of the same tests above: X-ray and MRI to make sure there's nothing more obvious going on. Maybe PT will be required, and even orthotics which I will discuss in treatment. Some doctors may even order blood tests to check and make sure all those numbers are in the normal range.
Stryker Test
It is not easy to get to the point where you actually have a doctor order the "Gold Standard" Stryker test. The Stryker test involves a hand held device that measures pressure in the 4 different compartments. Essentially you are going to have needles jabbed into your compartments before and after exercise as I mentioned above and then if your reading is above a certain number? Boom, you have compartment syndrome and they line you up for a pretty invasive surgery. It was incredibly difficult for me to get a Stryker test due to covid, but finally my best friend, who is an orthopedic surgeon, told me to drive 3 hours to her and that she would do the test. She doesn't perform them often and did everything right but noticed that the pressure reader was so sensitive. My pressure was already high enough for a CECS diagnosis before exercise and it barely elevated or changed after exercise so Chronic exertional Compartment Syndrome theoretically should get worse upon exertion and while my symptoms got worse, the pressure in my compartments didn’t rise. I’m not sure if this happens to all people with fPAES, but these results were strange. Since it was my best friend she didn’t want me to get surgery yet even though technically my numbers were high enough to indicate that was the next step, she did not like the results or the surgical outcomes for me and recommended I check with vascular before getting surgery since PAES was already on my radar. At the time all I wanted was a surgery, but she told me the outcomes of both surgeries weren’t good. I felt deflated because the only options on the table were either bad outcome surgeries or sedentary life. I was willing to take my chances with surgery because my symptoms were getting pretty severe that walking was pretty painful. I was having trouble getting anyone to see me due to COVID but eventually got in with vascular to see about PAES. I wont get into the craziness once I was on the vascular track as it's all in my blog, but all this to say, the Stryker test showed compartment syndrome, but my doctor felt that it wasn’t accurate or a reliable test due to pressure staying the same after exertion.

During the vascular mess, I spent a lot of time waiting for appointments. I joined a Facebook support group for CECS and PAES after my Stryker test to see if anyone else experienced that. I had seen Dr. McGinleys name come up a lot and attended his webinar while I was waiting for Covid numbers to go down so that I could get my intravenous ultrasound. It was scheduled for May, it was currently January. (I'm in Massachusetts and the hospitals could not always accommodate elective procedures depending on the case numbers, cases were really high in the winter) and learned that he had tested the Stryker test in a piece of meat or steak or something, and after a day of using it and recording numbers, he realized it was not accurate at all and that theres actually some bias to it since he could produce high or low pressure readings depending on how fast or slow he inserted needle (or something...? I don't know the details just that he's not a fan of the "Gold Standard")
Pre and Post exercise MRI's:
Dr. McGinley uses a pre and post test MRI to determine if someone has compartment syndrome. I got an MRI before running on a treadmill, ran on a treadmill and had symptoms recorded during the run, and then after 10 minutes (or for me 9:30 because I couldn't run anymore) I did a second MRI and it showed edema and swelling consistent with compartment syndrome. This is a much less invasive way to test and hopefully will be the "new" Gold Standard.
Pre and Post exercise MRI's:
Dr. McGinley uses a pre and post test MRI to determine if someone has compartment syndrome. I got an MRI before running on a treadmill, ran on a treadmill and had symptoms recorded during the run, and then after 10 minutes (or for me 9:30 because I couldn't run anymore) I did a second MRI and it showed edema and swelling consistent with compartment syndrome. This is a much less invasive way to test and hopefully will be the "new" Gold Standard.
Treatment
I'm just going to quickly run through a bunch of things I've tried that focused more on symptoms, and my take on them, and then I'll get into more specific treatment.
Modified Exercise -Yes, this is actually treatment, and it can get you a long way. Take necessary days off for recovery and decrease the activities that bring on the worst symptoms.
Massage and Foam Rolling- I Highly recommend doing these things to keep symptoms at bay. They help for sure, but ultimately, if you want to continue to do your sport these are just ways to pacify the problem not actually treat it... but again, you can manage for a while with this.
Epsom Salt Baths- Anecdotally, ice never seemed to relieve my symptoms, but warm baths for sure did. I would try ice but if compartment syndrome is from compressed veins, ice adds to the constriction of blood flow. I would try a contrast bath alternating between cold and hot if you want to get the most out of icing.
KT Tape- People can call this a placebo effect all they want, but in my experience this stuff really works... and placebo effects are still an effect so try it out.
Physical Therapy- If improving your efficiency and gait can change and improve symptoms, PT is the way to go.... but unfortunately it can make it worse if you are prescribed calf raises... which is likely if you have yet to receive a diagnosis.
Compression socks-Jury is out on this. Sometimes I swore by them, other times I thought they caused all my problems. Worth a cheap try.
Change in footwear- In my experience a stiffer shoe with more support allowed me to train way beyond the point any person in my condition should have trained, it helped! (didn't cure but helped)
Custom Orthotics-This is probably the single most effective thing I did to relieve symptoms. I don't know if I permanently need orthotics, but that firmness preventing me from intense plantar flexion helped
Shockwave Therapy- I loved this. It definitely helped my foot heal once it had some damage. It relieved symptoms more than treated the cause, but relieving symptoms allowed me to continue work and not have to take a leave of absence (yes, it was getting that bad. Weirdly covid helped me because teaching remotely allowed me to stay off my feet and so I was in less pain)
Acupuncture, Dry Needling, and cupping- I can't confidently say I got relief from any of these treatments. But tried them all. If I had to choose, Cupping and Dry Needling were covered by insurance under my PT, so Acupuncture I'd pass on.
Tens Machine- Temporary good feeling... but that's about it.
Compression Boots- I have them, probably more money than they are worth...
Thera-gun or trigger point guns- Late addition to my line up, I quite like mine. I feel like this helps a bit.... But another one of those "not great bank for your buck"
Modified Exercise -Yes, this is actually treatment, and it can get you a long way. Take necessary days off for recovery and decrease the activities that bring on the worst symptoms.
Massage and Foam Rolling- I Highly recommend doing these things to keep symptoms at bay. They help for sure, but ultimately, if you want to continue to do your sport these are just ways to pacify the problem not actually treat it... but again, you can manage for a while with this.
Epsom Salt Baths- Anecdotally, ice never seemed to relieve my symptoms, but warm baths for sure did. I would try ice but if compartment syndrome is from compressed veins, ice adds to the constriction of blood flow. I would try a contrast bath alternating between cold and hot if you want to get the most out of icing.
KT Tape- People can call this a placebo effect all they want, but in my experience this stuff really works... and placebo effects are still an effect so try it out.
Physical Therapy- If improving your efficiency and gait can change and improve symptoms, PT is the way to go.... but unfortunately it can make it worse if you are prescribed calf raises... which is likely if you have yet to receive a diagnosis.
Compression socks-Jury is out on this. Sometimes I swore by them, other times I thought they caused all my problems. Worth a cheap try.
Change in footwear- In my experience a stiffer shoe with more support allowed me to train way beyond the point any person in my condition should have trained, it helped! (didn't cure but helped)
Custom Orthotics-This is probably the single most effective thing I did to relieve symptoms. I don't know if I permanently need orthotics, but that firmness preventing me from intense plantar flexion helped
Shockwave Therapy- I loved this. It definitely helped my foot heal once it had some damage. It relieved symptoms more than treated the cause, but relieving symptoms allowed me to continue work and not have to take a leave of absence (yes, it was getting that bad. Weirdly covid helped me because teaching remotely allowed me to stay off my feet and so I was in less pain)
Acupuncture, Dry Needling, and cupping- I can't confidently say I got relief from any of these treatments. But tried them all. If I had to choose, Cupping and Dry Needling were covered by insurance under my PT, so Acupuncture I'd pass on.
Tens Machine- Temporary good feeling... but that's about it.
Compression Boots- I have them, probably more money than they are worth...
Thera-gun or trigger point guns- Late addition to my line up, I quite like mine. I feel like this helps a bit.... But another one of those "not great bank for your buck"
As you can see I tried a lot. That probably doesn't even include it all, but after lisening to McGinleys webinar I knew I needed to try botox next. At this point I knew that the surgeries were not good outcomes nearly half of the time, and that many people needed revisions. He described the calves like a tourniquet to arteries. The best option is to remove the tourniquet. The way McGinley does this is through botox.
McGinley Method (Botox)-Dr. McGinley uses the botox in a precise and patented manner and has very patient specific injection points. Botox is used by other Doctors as well but it is not the same method as his. He uses CT and Ultrasound to guide him instead of injecting into painful areas. People do report relief from other using Botox from other Doctors as well, Botox numbs and paralyzes muscle so theres temporary relief (numbing painful areas for long periods of time) but this method has less permanence. Dr. McGinley numbs the specific areas causing entrapment and then overtime they atrophy due to limited use. The goal is to numb muscles for a long enough period of time that a. They atrophy and b. Your body stops relying on them and everything. When the Botox wears off they aren’t problematic anymore.
He averages 2.7 treatments (possible touch ups needed between treatment 1 and 2 are not included in that 2.7 number) and after that people often don’t need to come back! I loved the diagnostic experience and highly recommend it, especially for the simplicity- skip all the steps above- the Mcginley clinic knows what to do and makes everyone else you’ve seen so far look like foolish chumps because they make it easy.
(This section updated August 2022)
My Progress: In a nutshell, as much as I still recommend it, it wasn’t exactly what I expected or hoped. I had immediate relief from the day to day pain about 4 days after my first treatment in April 2021. My legs were warm for the first time… ever… and pain that I didn’t even know existed was gone. I lived in more pain than I knew until the treatment made me realize what “normal” was like. The immediate relief made me really hopeful for running. Unfortunately, I still had the same sharp symptoms running even after only a few minutes. I went back for a touch up treatment (needing another treatment w/in 90 days) and even then I still had symptoms. I couldn’t even walk/run with 1 minute runs without jarring sharp pain. At this point I thought for sure it was related to nerves and I had an EMG which was normal… Everything I’ve read on nerves suggested that they sometimes just need time so I basically rested and hoped everything was healing below the surface. Seven months after first treatment (4 months after second) I consulted on the phone with McGinley and tried to run again. It was working! I ran 2-5 miles every other day! However 1.5 months after returning to running symptoms came back (Botox likely wore off). I got a third treatment with xeomin on the last day of Februar and was able to run the Boston marathon (slowly) 6 weeks later. I’d mostly call that a success! I still have a long way to go as it has been hard to adjust to the changes in my legs in addition to the weight I gained in the interim, but I am happy with the treatment so far.
It requires commitment, trust, patience, and either disposable income or a really good credit score! I’m happy with my decision and absolutely recommend McGinley and the team, but for transparency it’s definitely not as easy as it feels like it should be when you’re in the office and I think I would have handled it all better emotionally if I saw it less as a quick fix and more as a long journey of trust. It has absolutely been worth it for me, but ultimately it’s your decision! (more on this discussed in surgery section.)
He averages 2.7 treatments (possible touch ups needed between treatment 1 and 2 are not included in that 2.7 number) and after that people often don’t need to come back! I loved the diagnostic experience and highly recommend it, especially for the simplicity- skip all the steps above- the Mcginley clinic knows what to do and makes everyone else you’ve seen so far look like foolish chumps because they make it easy.
(This section updated August 2022)
My Progress: In a nutshell, as much as I still recommend it, it wasn’t exactly what I expected or hoped. I had immediate relief from the day to day pain about 4 days after my first treatment in April 2021. My legs were warm for the first time… ever… and pain that I didn’t even know existed was gone. I lived in more pain than I knew until the treatment made me realize what “normal” was like. The immediate relief made me really hopeful for running. Unfortunately, I still had the same sharp symptoms running even after only a few minutes. I went back for a touch up treatment (needing another treatment w/in 90 days) and even then I still had symptoms. I couldn’t even walk/run with 1 minute runs without jarring sharp pain. At this point I thought for sure it was related to nerves and I had an EMG which was normal… Everything I’ve read on nerves suggested that they sometimes just need time so I basically rested and hoped everything was healing below the surface. Seven months after first treatment (4 months after second) I consulted on the phone with McGinley and tried to run again. It was working! I ran 2-5 miles every other day! However 1.5 months after returning to running symptoms came back (Botox likely wore off). I got a third treatment with xeomin on the last day of Februar and was able to run the Boston marathon (slowly) 6 weeks later. I’d mostly call that a success! I still have a long way to go as it has been hard to adjust to the changes in my legs in addition to the weight I gained in the interim, but I am happy with the treatment so far.
It requires commitment, trust, patience, and either disposable income or a really good credit score! I’m happy with my decision and absolutely recommend McGinley and the team, but for transparency it’s definitely not as easy as it feels like it should be when you’re in the office and I think I would have handled it all better emotionally if I saw it less as a quick fix and more as a long journey of trust. It has absolutely been worth it for me, but ultimately it’s your decision! (more on this discussed in surgery section.)

Baseline
|
While Botox is still active

After Botox has worn off (big improvement from baseline!)

|
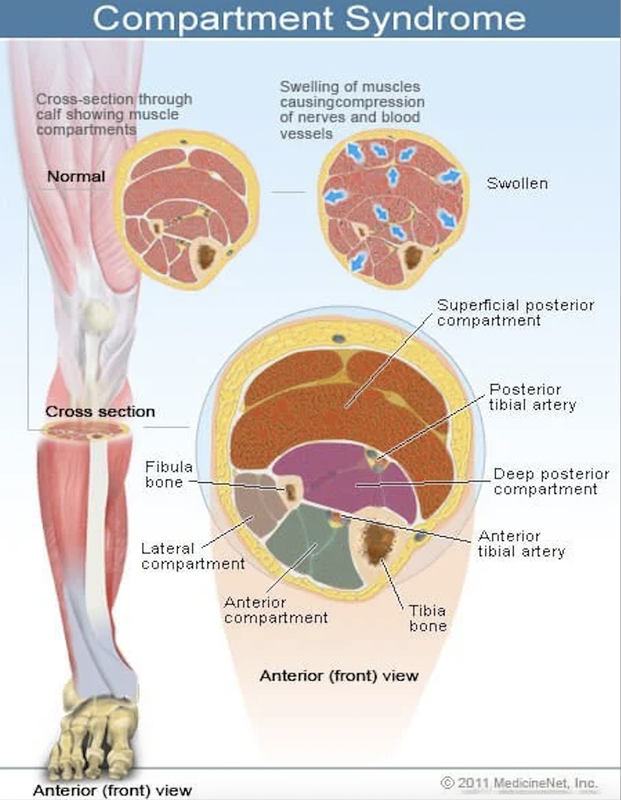
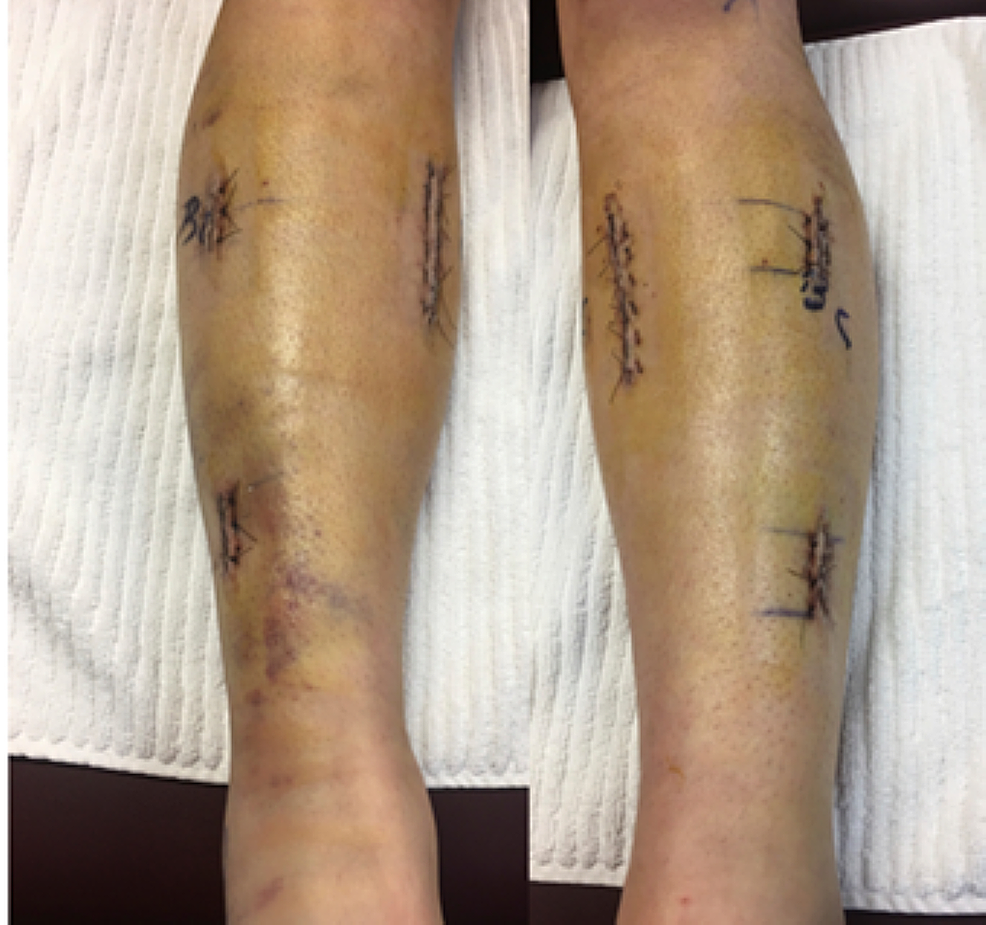
Surgery: The surgeries for CECS and fPAES are different because they are largely seen as different problems. In general CECS falls under the orthopedic scope, and fPAES falls under the vascular scope, however McGinleys research is showing that in many cases they are both vascular. Typically CECS is treated with a fasciotomy or a fasciectomy. This procedure is highly invasive and carries a great risk of infection. It basically slices the fascia in order to relive the pressure that is theoretically caused by smaller compartments. However, according to Doctor McGinleys research it's due to a mismatch of pressure and starling forces. If Veins are entrapped then blood can not travel back up through the popliteal fossa at the same rate that it is traveling down through the arteries. This is a much more logical reason for why the pressure builds upon exertion. Fasciotomies and Faciectomies are effective and necessary for acute compartment syndrome (cased from blunt force such as car accident). But for Chronic Exertional Compartment Syndrome, the anterior compartment has the best outcomes, but for other compartments, especially the deep posterior, symptoms often return and revisions are needed. I know many people that have had the surgeries and have been successful. Some needed revisions, but overall it is pretty intense and leave big scars so not something to take lightly or rush into especially when it might be treating the symptom not the underlining cause. Here are sample scars from compartment syndrome:
|

|
Surgery for fPAES is different. Typically you see a scar in the shape of an S behind the knee. It seems as though surgeons have to guess how much muscle to remove in order to free up space for the arteries and veins. (and nerve). Most of what I read says the doctor cuts the plantaris completely out, and additionally may cut out the soleal sling. In many cases the more aggressive the doctor is cutting out muscle, the more effective the surgeries tend to be. Less aggressive may need revisions. Some patients may even be given a stent or a bypass or vascular reconstruction depending on the surgeon. For transparency, I never had any surgeries, so I can’t give a full picture of it. Some recoveries I've seen go real smoothly, some are really hard... I’m going to discuss the factors that led me to me decision so you can consider them making yours.

There were a lot of factors I considered and why I got Botox.
a. I didn’t have a diagnosis and we were deep into Covid. Wyoming politics helped me out because the state was wide open whine elective procedures were impossible in my area
b. I didn’t like seeing so many negative outcomes with such an invasive surgery, I recognize that support groups are an echo chamber of people that haven’t resolved symptoms yet, so it was a bit one sided information, but what I was seeing had me really pumping the brakes on surgery (which I would have done in the blink of an eye prior to attending the McGinley webinar)
c. this is a long term commitment and since my job is physical, it would put me out of work for multiple surgeries. I also have small children so proper recovery as a mom seemed impossible. Neither of my kids are independent and my husbands work requires a lot of travel so it was going to effect his work as well. (I just kept picturing my youngest jumping on my legs as I lay down on the couch. No thanks!)
d. It’s still going to be expensive… which I’ll break down next.
At first, it seems like it could potentially be cheaper since insurance is more likely to cover surgery (McGinleys is not covered because it’s not FDA approved) however you will definitely want to look thoroughly into what is involved to make the best decision for yourself. I personally would want to have the absolute best surgeon because I really think that makes the difference based on those I’ve talked to who had successful operations. I had my eyes on Dr Lyden from the Cleveland Clinic and Dr. Sarkar who I believe is in the DC area (can’t remember)… It is very unlikely any surgeon would do both legs at a time(and you probably don’t want that from what I understand, anyway) so it would be two trips at a minimum (not including potential consults etc.) Fir me, personally, both doctors were out of my network, require flying, would require overnight hospital stays AND hotel stays for a caretaker (which you would need navigating the airport etc. after procedure) and depending on your work benefits, more time off… so consider all those costs when you think surgery is “cheaper”… It’s a difficult diagnosis it can be limb threatening (mentioned below) but not life threatening so patience is key no matter what treatment option is Selected.
a. I didn’t have a diagnosis and we were deep into Covid. Wyoming politics helped me out because the state was wide open whine elective procedures were impossible in my area
b. I didn’t like seeing so many negative outcomes with such an invasive surgery, I recognize that support groups are an echo chamber of people that haven’t resolved symptoms yet, so it was a bit one sided information, but what I was seeing had me really pumping the brakes on surgery (which I would have done in the blink of an eye prior to attending the McGinley webinar)
c. this is a long term commitment and since my job is physical, it would put me out of work for multiple surgeries. I also have small children so proper recovery as a mom seemed impossible. Neither of my kids are independent and my husbands work requires a lot of travel so it was going to effect his work as well. (I just kept picturing my youngest jumping on my legs as I lay down on the couch. No thanks!)
d. It’s still going to be expensive… which I’ll break down next.
At first, it seems like it could potentially be cheaper since insurance is more likely to cover surgery (McGinleys is not covered because it’s not FDA approved) however you will definitely want to look thoroughly into what is involved to make the best decision for yourself. I personally would want to have the absolute best surgeon because I really think that makes the difference based on those I’ve talked to who had successful operations. I had my eyes on Dr Lyden from the Cleveland Clinic and Dr. Sarkar who I believe is in the DC area (can’t remember)… It is very unlikely any surgeon would do both legs at a time(and you probably don’t want that from what I understand, anyway) so it would be two trips at a minimum (not including potential consults etc.) Fir me, personally, both doctors were out of my network, require flying, would require overnight hospital stays AND hotel stays for a caretaker (which you would need navigating the airport etc. after procedure) and depending on your work benefits, more time off… so consider all those costs when you think surgery is “cheaper”… It’s a difficult diagnosis it can be limb threatening (mentioned below) but not life threatening so patience is key no matter what treatment option is Selected.
Amputation: I have to mention it because I know three people from the support group that had amputation. Over time the artery can get damaged and if it gets damaged enough that there is a dissection, or the artery frays, it can get really serious really fast. Additionally, When the surgeries fail sometimes they leave scar tissue that press on the nerves and cause more pain. Sometimes there's infections, and sometimes people are just in so much pain and so tired it seems like the easier option. Not a fun reality, but it is a reality… one that, if you’re like me, you maybe already considered as a possibility before getting a diagnosis. It is considered the worst outcome of this condition but it does seem to be rare. As we all know, though… rare doesn’t mean impossible so thought I should include this and hope it’s not triggering. I worried a lot about this prior to my diagnosis, but I no longer worry about this for myself.
My McGinley Experience: Hope this was helpful! If you would like to read even more details about how my experience with the McGinley Method has been, the journey starts here. Apologies in advance, there continue to be glitches with the blogposts and photos. Sometimes old photos appear in new posts and vice versa, I’m working on fixing them and of I haven’t updated in a while, I will! Or find me on instagram! @caitlyn_germain_
Disclaimer: This is not meant to be medical advice, I'm just sharing personal anecdotes.